Introduction: Why Diabetic Foot Infections Are a Serious Concern
Diabetes is a complex metabolic condition that affects virtually every system in the human body. Among its many complications, foot infections stand out as one of the most dangerous and frequently overlooked. Each year, diabetic foot infections lead to thousands of hospitalizations and, in the most severe cases, amputations. In fact, diabetes is the leading cause of non-traumatic lower-limb amputations worldwide.
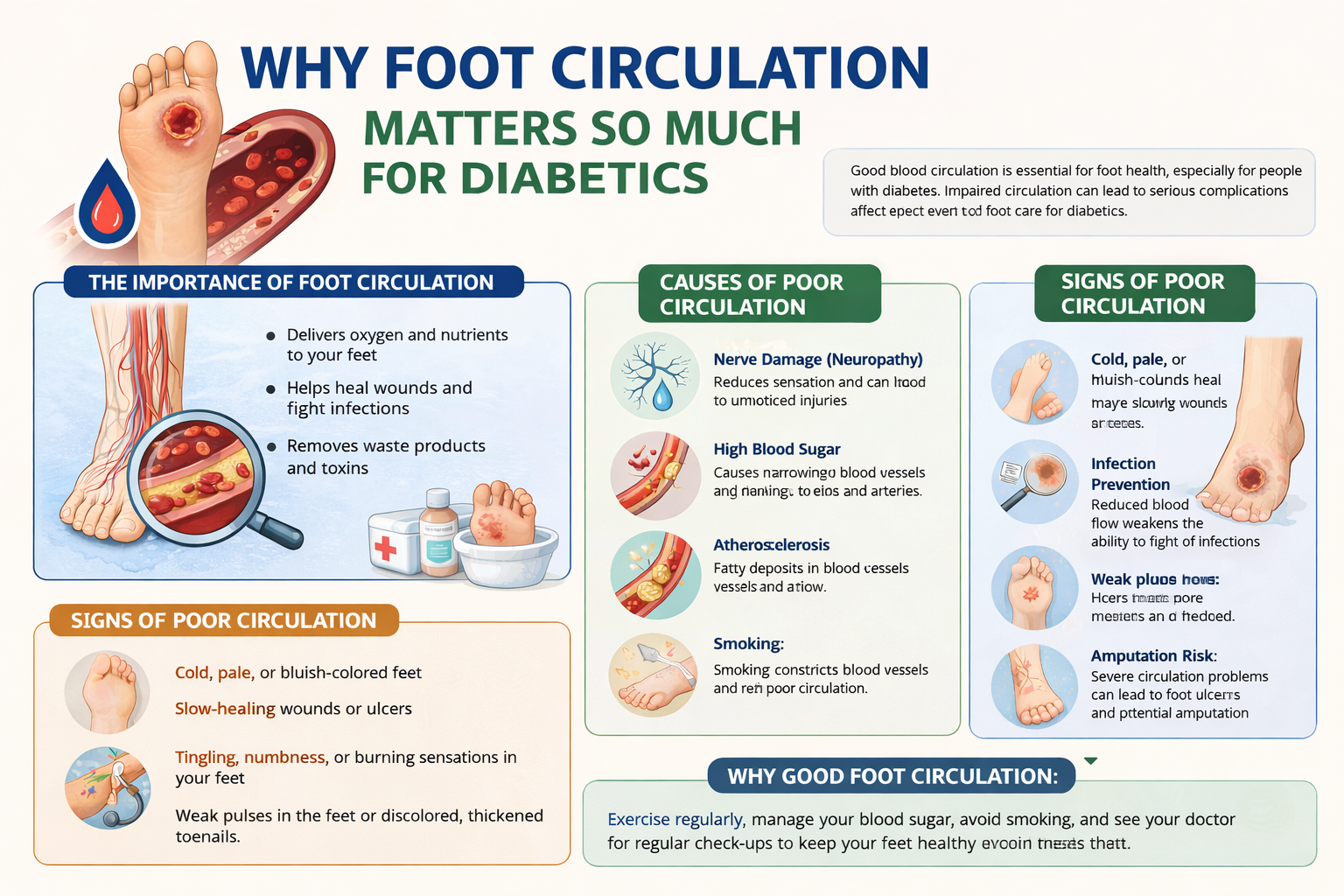
What makes diabetic foot infections particularly treacherous is the insidious way they develop. Because diabetes can cause nerve damage (neuropathy) and reduce blood flow to the extremities, many patients simply don’t feel the early warning signs — a small blister, a tiny cut, or a seemingly minor sore. By the time the infection becomes noticeable, it may have already penetrated deep into the tissue, bone, or bloodstream.
Understanding the warning signs of diabetic foot infections and knowing the treatment options available could literally save your life — or at the very least, save your limb. In this comprehensive guide, we’ll walk you through everything you need to know about diabetic foot infections, from why they occur to how they’re treated and prevented.
Understanding the Connection Between Diabetes and Foot Problems
To fully appreciate why diabetic foot infections are so dangerous, it’s important to understand the underlying mechanisms that make people with diabetes more vulnerable to foot problems in the first place.
Peripheral Neuropathy: The Silent Thief of Sensation
High blood sugar levels over time can damage the nerves throughout the body, a condition known as peripheral neuropathy. When the nerves in the feet are affected, patients may experience tingling, burning, or numbness. This loss of sensation means that minor injuries — a pebble in the shoe, a tight-fitting sock, a small cut from toenail trimming — go undetected and untreated. Without proper attention, even the smallest wound can become an open gateway for bacteria.
Peripheral Arterial Disease: Reduced Blood Flow
Diabetes also damages blood vessels, particularly in the extremities. Peripheral arterial disease (PAD) reduces blood flow to the feet, meaning that even when an infection does occur, the body’s immune cells and oxygen-rich blood cannot reach the area efficiently. This impairs the natural healing process and allows infections to spread more rapidly. Wounds that would heal in days for a healthy person might linger for weeks or months in a diabetic patient.
Immune System Dysfunction
High blood glucose levels can impair the function of white blood cells, the body’s primary defense against infection. When these cells can’t work properly, even common bacteria like Staphylococcus aureus or Streptococcus can overpower the body’s defenses and cause serious infections. This immune dysfunction, combined with neuropathy and poor circulation, creates a perfect storm for foot infections in diabetic patients.
Warning Signs of Diabetic Foot Infection
Early detection is absolutely critical when it comes to diabetic foot infections. Recognizing the signs — even subtle ones — can mean the difference between a simple course of antibiotics and a life-altering amputation. Here are the most important warning signs to watch for:
1. Redness and Warmth Around the Foot or Wound
One of the earliest signs of a developing infection is localized redness (erythema) around a wound, sore, or ulcer. The skin may feel warm to the touch compared to surrounding areas. This indicates that the immune system is responding to bacteria, and inflammation has begun. Even if the area is painless due to neuropathy, visible redness should never be dismissed.
2. Swelling
Swelling in the foot, ankle, or lower leg — especially when concentrated around a wound — is a classic sign of infection. The affected area may appear puffy, distended, or larger than normal. Bilateral swelling (in both feet equally) is more commonly associated with fluid retention or vascular issues, but unilateral or localized swelling around a wound is a red flag for infection.
3. Discharge or Pus
The presence of any discharge from a wound is a significant warning sign. Infected wounds may produce pus, which can range in color from pale yellow to green or brown. A foul or unusual odor accompanying the discharge is especially concerning, as it may indicate anaerobic bacteria — organisms that thrive in low-oxygen environments like deep tissue wounds.
4. Slow-Healing or Non-Healing Wounds and Ulcers
Diabetic foot ulcers are open sores that commonly develop on the bottom of the foot. When a wound or ulcer fails to show signs of healing within two weeks, or when it continues to grow despite treatment, this may indicate an underlying infection. Chronic non-healing wounds are among the most common entry points for serious diabetic foot infections.
5. Fever and Chills
Systemic symptoms like fever (temperature above 100.4°F or 38°C), chills, sweating, or general malaise indicate that the infection may have entered the bloodstream — a condition called sepsis. This is a medical emergency that requires immediate hospitalization. Importantly, some diabetic patients may not exhibit a fever even with severe infections due to immune dysfunction, so the absence of fever doesn’t rule out a serious infection.
6. Pain or Increased Sensitivity
While many diabetic patients with neuropathy experience reduced sensation, some may actually develop hypersensitivity (allodynia), where even light touch causes pain. New or changing pain in the foot, particularly around an existing wound, should be taken seriously. Paradoxically, if a previously painful wound suddenly becomes painless, this may indicate worsening neuropathy or tissue death rather than healing.
7. Skin Discoloration and Tissue Changes
Dark discoloration — bluish, purple, or black areas — around a wound or on the foot itself is extremely alarming. This may indicate tissue necrosis (gangrene), a condition in which tissue dies due to inadequate blood supply and severe infection. Gangrene requires emergency medical treatment and may necessitate surgical debridement or amputation to prevent the spread of infection.
8. Skin Breakdown and Blisters
Blisters, especially fluid-filled ones, can quickly become infected if they rupture. Similarly, calluses, corns, or areas of skin that crack and break open (fissures) create entry points for bacteria. Regular foot inspection is crucial to catch these issues before they escalate.
9. Foul Odor
A strong, unpleasant smell emanating from the foot — even without visible drainage — can be a warning sign of deep tissue infection or necrosis. Certain bacteria produce distinctive odors, and the presence of this symptom should prompt immediate medical evaluation.
10. Bone or Tendon Visibility
In severe cases, infection and tissue destruction may be extensive enough that bone, tendons, or deep structures become visible within a wound. This is a dire emergency indicating osteomyelitis (bone infection) or severe necrotizing fasciitis and requires immediate surgical intervention.
How Diabetic Foot Infections Are Classified
Medical professionals use standardized classification systems to assess the severity of diabetic foot infections and guide treatment decisions. The most widely used system is the Infectious Diseases Society of America (IDSA) classification, which categorizes infections as follows:
- Uninfected: A wound with no signs of infection. No systemic or local signs of inflammation are present.
- Mild Infection: Local infection involving only the skin and subcutaneous tissue. Characterized by redness, warmth, swelling, or discharge, but no systemic illness.
- Moderate Infection: Infection extending deeper than the skin — into muscle, tendon, joint, or bone — but without systemic toxicity.
- Severe Infection: Any foot infection accompanied by systemic signs of illness such as fever, chills, elevated heart rate, low blood pressure, or high white blood cell count.
This classification system helps clinicians determine whether a patient can be managed with oral antibiotics at home, requires intravenous antibiotics, or needs emergency hospitalization and surgical intervention.
Diagnosing a Diabetic Foot Infection
Accurate diagnosis is essential for effective treatment. Healthcare providers use a combination of clinical examination and diagnostic tests to assess the extent of a diabetic foot infection.
Physical Examination
A thorough physical examination includes inspecting the wound for size, depth, tissue color, drainage, and odor. The doctor will probe the wound to assess its depth and check whether bone can be felt — a technique called the “probe-to-bone” test, which has a high predictive value for osteomyelitis. Vascular assessments such as checking pedal pulses help evaluate blood flow to the area.
Blood Tests
Laboratory tests including a complete blood count (CBC), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and blood glucose levels help identify signs of systemic infection and inflammation. Blood cultures may also be drawn to identify organisms in the bloodstream in cases of suspected sepsis.
Wound Cultures
Deep tissue cultures taken from the base of the wound (not surface swabs) help identify the causative microorganisms and their antibiotic sensitivities. This information is crucial for choosing the right antibiotic therapy. Diabetic foot infections are often polymicrobial, meaning they involve multiple types of bacteria.
Imaging Studies
X-rays are typically the first imaging study ordered, as they can reveal bone destruction indicative of osteomyelitis, gas within soft tissues (suggesting gas-forming bacteria), or foreign bodies. For a more detailed evaluation, MRI (magnetic resonance imaging) is the gold standard for detecting soft tissue infections and osteomyelitis. In some cases, bone scans or CT scans may also be used.
Treatment Options for Diabetic Foot Infections
Treatment for diabetic foot infections depends on the severity of the infection, the patient’s overall health, the presence of underlying conditions like PAD, and whether there is involvement of deep structures like bone or tendon. A multidisciplinary approach — involving endocrinologists, infectious disease specialists, vascular surgeons, podiatrists, and wound care nurses — often yields the best outcomes.
1. Wound Care and Debridement
Proper wound care is the foundation of diabetic foot infection management. This involves cleaning the wound thoroughly, removing dead or infected tissue through a process called debridement, and applying appropriate dressings to promote healing. Debridement can be performed surgically, mechanically (using wet-to-dry dressings), enzymatically (with special dressings), or biologically (using maggot therapy in some specialized centers).
Regular dressing changes and moisture management are essential. Modern wound dressings — such as hydrocolloids, foam dressings, silver-impregnated dressings, and biofilm-disrupting agents — help manage infection, reduce exudate, and create an optimal healing environment.
2. Antibiotic Therapy
Antibiotics are a cornerstone of diabetic foot infection treatment. The choice of antibiotic depends on the severity of the infection, likely organisms, local resistance patterns, and results from wound cultures.
- Mild infections: Often treated with oral antibiotics targeting common skin organisms like Staphylococcus aureus and Streptococcus. Common choices include cephalexin, amoxicillin-clavulanate, or clindamycin.
- Moderate to severe infections: Typically require broad-spectrum intravenous antibiotics to cover gram-positive, gram-negative, and anaerobic organisms. Options may include piperacillin-tazobactam, vancomycin (for MRSA coverage), or carbapenem antibiotics in resistant cases.
- Osteomyelitis: Bone infections usually require prolonged antibiotic therapy — often 4 to 6 weeks or longer — with IV antibiotics followed by oral step-down therapy.
Antibiotic-resistant organisms, particularly MRSA (Methicillin-resistant Staphylococcus aureus), are an increasing concern in diabetic foot infections and must be considered, especially in patients with prior antibiotic exposure or healthcare exposure.
3. Offloading and Pressure Relief
Continuous pressure on an infected or ulcerated foot dramatically impairs healing and can worsen tissue damage. Offloading — removing mechanical pressure from the affected area — is a critical but often underappreciated aspect of treatment. Options include:
- Total Contact Cast (TCC): Considered the gold standard for offloading diabetic foot ulcers. It distributes pressure evenly across the entire foot and cannot be easily removed, ensuring compliance.
- Removable Cast Walkers (RCWs): Prefabricated boots that can be removed for wound inspection and bathing, though compliance can be an issue.
- Custom Therapeutic Footwear: Special shoes with custom insoles designed to redistribute pressure away from vulnerable areas.
- Crutches or Wheelchairs: Used when absolute non-weight-bearing is necessary.
4. Revascularization for Peripheral Arterial Disease
In many patients with diabetic foot infections, underlying peripheral arterial disease significantly impairs healing. Without adequate blood flow, antibiotics cannot reach the infection site effectively, and tissue healing is severely compromised. In these cases, revascularization — restoring blood flow to the foot — may be necessary before wound healing can occur.
Revascularization procedures include:
- Angioplasty and stenting: A minimally invasive procedure where a balloon catheter opens blocked arteries and a stent is placed to keep them open.
- Bypass surgery: A surgical procedure that creates a new route for blood flow around a blocked artery using a graft vessel.
A vascular surgery consultation is essential in any diabetic foot infection patient with signs of poor circulation.
5. Surgical Intervention
Surgery is often required in moderate to severe diabetic foot infections. Surgical options range from minor procedures to major interventions:
- Incision and Drainage (I&D): Opening an abscess to drain pus and relieve pressure. This is often the first step in surgical management.
- Surgical Debridement: Removal of infected, necrotic, or non-viable tissue to create a clean wound bed. This may need to be repeated in stages.
- Sesamoidectomy or bone resection: Removal of bony prominences or infected bone segments to reduce pressure points and eliminate osteomyelitis.
- Amputation: In cases of severe infection, uncontrollable gangrene, or life-threatening sepsis, amputation may be necessary. The goal is always to perform the most distal (lowest-level) amputation possible — preserving as much of the foot and limb as feasible. This may range from a toe amputation to a transmetatarsal amputation, below-knee amputation, or in the worst cases, above-knee amputation.
6. Advanced Wound Care Technologies
Several advanced wound care modalities can enhance healing in diabetic foot infections:
- Negative Pressure Wound Therapy (NPWT): Also known as vacuum-assisted closure (VAC) therapy, this technique uses controlled suction to remove fluid and infectious material, reduce swelling, and stimulate new tissue growth. It is widely
Categories: