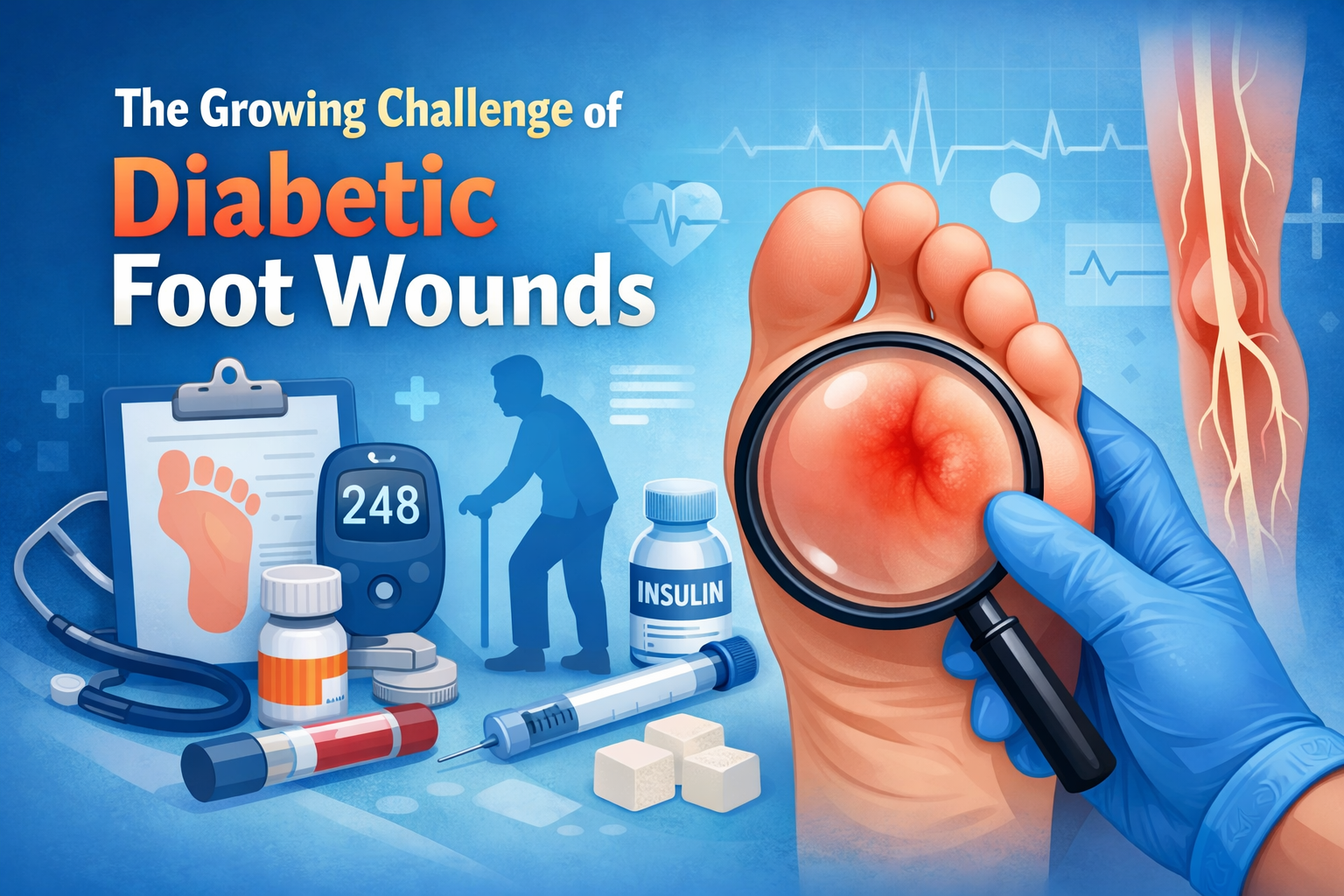
Introduction: The Growing Challenge of Diabetic Foot Wounds
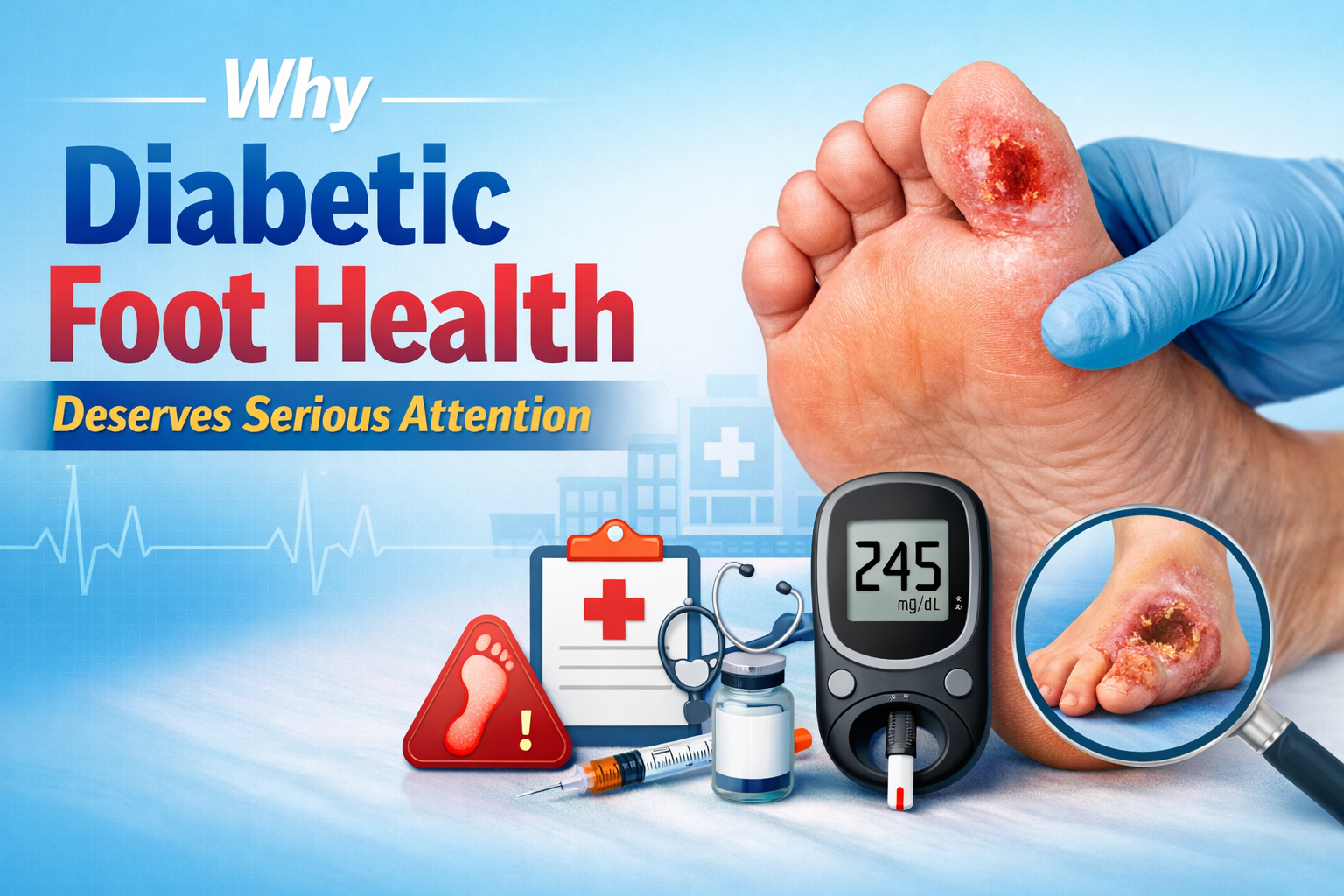
Diabetic foot wounds represent one of the most serious and complex complications associated with diabetes mellitus. Globally, more than 537 million people are living with diabetes, and an alarming 15 to 25 percent of them will develop a foot ulcer at some point during their lifetime. These wounds are notoriously difficult to heal due to the underlying physiological damage caused by chronic high blood sugar — including nerve damage (neuropathy), poor circulation (peripheral arterial disease), and a compromised immune response.
Left untreated or poorly managed, diabetic foot ulcers can rapidly progress to deep tissue infection, osteomyelitis (bone infection), gangrene, and ultimately, lower limb amputation. In fact, diabetes is the leading cause of non-traumatic lower limb amputations worldwide. The human cost is devastating — and the economic burden is equally staggering, with billions of dollars spent annually on diabetic foot care.
However, the landscape of wound care has transformed dramatically over the past two decades. Today, a rich arsenal of advanced, evidence-based treatments is available to clinicians and patients alike. From bioengineered skin substitutes and growth factor therapies to hyperbaric oxygen chambers and regenerative medicine, modern wound care offers genuine hope for healing even the most stubborn diabetic foot wounds. This article takes an in-depth look at these cutting-edge treatments, how they work, and when they are most effective.
Understanding Why Diabetic Foot Wounds Are So Difficult to Heal
Before diving into advanced treatments, it’s important to understand the biological and physiological barriers that make diabetic foot wounds so uniquely challenging. This context helps explain why conventional wound care alone is often insufficient.
Peripheral Neuropathy
High blood glucose levels over time damage the peripheral nerves, particularly in the feet and lower legs. This leads to a loss of protective sensation, meaning patients cannot feel pain, pressure, or injury. A small blister, a pebble in a shoe, or a minor cut can go unnoticed for days or even weeks, allowing damage to accumulate without intervention. Motor neuropathy also causes foot deformities that create abnormal pressure points, while autonomic neuropathy reduces sweat production, leaving skin dry and prone to cracking.
Peripheral Arterial Disease (PAD)
Diabetes accelerates atherosclerosis — the hardening and narrowing of blood vessels. Reduced arterial blood flow to the feet means tissues receive less oxygen and fewer nutrients, both of which are critical for wound healing. It also means that antibiotics and immune cells have difficulty reaching the site of infection. Without adequate perfusion, even minor wounds struggle to heal.
Impaired Immune Function
Chronic hyperglycemia impairs neutrophil and macrophage function — the key immune cells responsible for fighting infection and initiating the healing process. This makes diabetic patients far more susceptible to infection and less capable of clearing bacteria from a wound once infection sets in.
Chronic Inflammation and Biofilm
Diabetic wounds are frequently trapped in a chronic inflammatory state. They fail to progress through the normal phases of wound healing (hemostasis, inflammation, proliferation, remodeling). Additionally, bacterial biofilms — structured communities of bacteria encased in a protective matrix — are present in up to 90 percent of chronic wounds, making them extraordinarily resistant to antibiotics and the body’s own immune defenses.
The Foundation: Standard Wound Care Practices
Advanced treatments are most effective when built upon a strong foundation of standard wound care. These foundational practices remain essential regardless of which advanced therapies are employed.
- Glycemic control: Optimizing blood sugar levels is non-negotiable. Poor glucose control undermines every other treatment effort.
- Debridement: The removal of dead, infected, or non-viable tissue from the wound bed is critical to preparing the wound for healing.
- Infection management: Identifying and treating infection with appropriate antibiotics, guided by culture results, is a priority.
- Offloading: Reducing pressure on the wound through specialized footwear, casts, or orthotic devices prevents further trauma and allows tissue to regenerate.
- Moist wound environment: Maintaining an optimal moisture balance with appropriate dressings supports cell migration and reduces infection risk.
- Vascular assessment and intervention: Restoring blood flow through revascularization procedures is often necessary before healing can occur.
Advanced Treatment 1: Negative Pressure Wound Therapy (NPWT)
Negative Pressure Wound Therapy, also known as vacuum-assisted closure (VAC) therapy, is one of the most widely adopted advanced wound care technologies in the world. It involves placing a specially designed foam or gauze dressing into the wound cavity, sealing it with an airtight film, and connecting it to a suction device that applies continuous or intermittent sub-atmospheric pressure to the wound.
How NPWT Works
The negative pressure created by the device accomplishes several therapeutic goals simultaneously. It removes excess wound fluid and exudate, which reduces edema and decreases the bacterial burden. The mechanical forces also stimulate cell proliferation and angiogenesis (the formation of new blood vessels), promoting the growth of healthy granulation tissue. NPWT also draws the wound edges together, reducing the wound’s surface area over time.
Clinical Evidence
Multiple randomized controlled trials have demonstrated that NPWT significantly accelerates wound healing, reduces the incidence of amputation, and shortens hospital stays in patients with diabetic foot ulcers compared to conventional moist wound therapy. It is particularly valuable for post-surgical wounds following debridement or partial foot amputations.
Newer Variations: NPWT with Instillation
An exciting evolution of traditional NPWT is negative pressure wound therapy with instillation and dwell time (NPWTi-d). This technology adds the ability to instill antiseptic or saline solutions directly into the wound cavity, allowing them to dwell for a set period before being removed by suction. This combination is particularly effective for heavily infected wounds and biofilm management, with studies showing reduced wound volume and faster progression to closure.
Advanced Treatment 2: Bioengineered Skin Substitutes
Bioengineered skin substitutes represent a revolutionary approach to wound closure. Rather than simply covering a wound, these products actively participate in the healing process by delivering living cells, growth factors, and structural scaffolding that the diabetic wound environment lacks.
Types of Skin Substitutes
- Cellular skin substitutes: These products contain living human cells — either allogeneic (donor-derived) keratinocytes and fibroblasts or xenogeneic (animal-derived) cells. Examples include Apligraf (a bilayered living skin equivalent containing both dermal and epidermal components) and Dermagraft (a cryopreserved human fibroblast-derived dermal substitute).
- Acellular skin substitutes: These are scaffolding products derived from human, animal, or synthetic sources that have been processed to remove cells, leaving behind the extracellular matrix (ECM). Examples include Oasis Wound Matrix (derived from porcine small intestinal submucosa) and Integra Dermal Regeneration Template.
- Amniotic membrane products: Derived from human placental tissue, these products are rich in growth factors, cytokines, and anti-inflammatory proteins. They are available in dehydrated, cryopreserved, and fresh forms and have shown impressive results in clinical trials.
How They Promote Healing
Skin substitutes work by delivering the biological signals and structural components that are deficient in chronic diabetic wounds. Cellular substitutes secrete growth factors such as PDGF, TGF-β, and VEGF that stimulate the patient’s own cells to proliferate and migrate. Acellular scaffolds provide a physical framework for host cell ingrowth and angiogenesis. Amniotic products modulate the inflammatory environment, reducing the chronic inflammation that blocks healing progression.
Clinical Results
Randomized clinical trials comparing bioengineered skin substitutes to standard care have consistently shown higher rates of complete wound closure, faster time to healing, and reduced amputation rates. Apligraf, for example, received FDA approval for diabetic foot ulcers based on trials showing significantly higher healing rates compared to standard care alone.
Advanced Treatment 3: Growth Factor Therapies
Growth factors are naturally occurring proteins that regulate cell behavior — including migration, proliferation, and differentiation — all of which are critical to wound healing. In diabetic wounds, the levels and activity of key growth factors are significantly reduced, contributing to the healing deficit.
Platelet-Derived Growth Factor (PDGF): Becaplermin
Becaplermin (brand name Regranex) is the only FDA-approved topical growth factor therapy for diabetic foot ulcers. It is a recombinant form of human PDGF-BB applied daily to the wound bed. PDGF stimulates the chemotaxis and proliferation of fibroblasts, neutrophils, and monocytes, promoting the formation of granulation tissue and wound closure.
Clinical trials demonstrated that becaplermin gel increased the incidence of complete wound healing by approximately 43 percent compared to placebo. However, its use has been somewhat limited by cost and concerns about a possible increased risk of malignancy with repeated tubes (though evidence remains inconclusive).
Platelet-Rich Plasma (PRP)
Platelet-Rich Plasma therapy involves drawing a small amount of the patient’s own blood, centrifuging it to concentrate the platelets, and then applying the platelet-rich concentrate directly to the wound. Activated platelets release a cocktail of growth factors including PDGF, TGF-β, VEGF, and EGF, creating a highly bioactive wound environment.
PRP therapy is autologous (derived from the patient’s own blood), making it safe and free from the risk of rejection or disease transmission. A growing body of evidence supports its use in diabetic foot ulcers, with several systematic reviews showing improved healing rates and reduced time to closure compared to standard care.
Epidermal Growth Factor (EGF)
Recombinant human EGF has been studied extensively, particularly in Asia and Latin America, for its ability to stimulate keratinocyte and fibroblast proliferation in diabetic foot wounds. Intralesional injection of EGF has shown particularly promising results, with studies demonstrating significant improvements in wound healing and limb salvage rates in patients with Wagner Grade 3 and 4 diabetic foot ulcers — wounds that would otherwise often require amputation.
Advanced Treatment 4: Hyperbaric Oxygen Therapy (HBOT)
Hyperbaric Oxygen Therapy involves placing a patient inside a pressurized chamber and having them breathe 100 percent pure oxygen at pressures greater than normal atmospheric pressure (typically 2 to 3 atmospheres absolute). This dramatically increases the amount of oxygen dissolved in the blood plasma and delivered to tissues.
Mechanisms of Action
The therapeutic benefits of HBOT for diabetic foot wounds are multifaceted and well-established:
- Enhanced tissue oxygenation: HBOT delivers 10 to 15 times more oxygen to hypoxic wound tissues than breathing room air, directly supporting cellular energy production and healing processes.
- Angiogenesis stimulation: Cycles of hyperoxia followed by relative hypoxia stimulate the release of VEGF, promoting the growth of new blood vessels into ischemic tissue.
- Enhanced antimicrobial activity: Many bacteria, including anaerobes, are killed by high-oxygen environments. HBOT also restores the oxidative burst killing mechanism of white blood cells, which is impaired in hyperglycemia.
- Reduced edema: The vasoconstrictive effect of HBOT reduces tissue edema without compromising oxygen delivery.
- Fibroblast and collagen synthesis: HBOT stimulates fibroblast proliferation and collagen production, strengthening the healing wound.
Clinical Applications and Evidence
HBOT is approved by the Centers for Medicare and Medicaid Services (CMS) for diabetic wounds of the lower extremity that have not responded adequately to 30 days of standard wound care. It is typically administered as daily sessions of 90 to 120 minutes, five days per week, for a total of 20 to 40 sessions.
Multiple systematic reviews and meta-analyses have concluded that HBOT significantly reduces the risk of major amputation in patients with ischemic diabetic foot wounds. The evidence is strongest for patients with concurrent peripheral arterial disease, where tissue oxygen levels are critically compromised. HBOT is most effective as an adjunct to, rather than a replacement for, other standard and advanced therapies.
Advanced Treatment 5: Biofilm Management and Advanced Antimicrobial Strategies
Given that biofilm is present in the vast majority of chronic diabetic foot wounds and is a primary driver of non-healing, targeted biofilm management has become a cornerstone of advanced wound care.
Biofilm Disruption Through Debridement
Regular and aggressive debridement — whether sharp surgical debridement, enzymatic debridement, or mechanical debridement — physically disrupts biofilm architecture. However, because biofilm reforms within 24 to 72 hours after debridement, repeated treatments are necessary. Ultrasonic debridement devices, which use low-frequency ultrasound waves to cavitate and disrupt biofilm while simultaneously irrigating the wound, have shown particular promise.
Antimicrobial Wound Dressings
A wide range of advanced antimicrobial dressings have been developed to address biofilm and infection in diabetic wounds:
- Ionic silver dressings: Silver ions are powerfully antimicrobial and effective against a broad spectrum of bacteria, including methicillin-resistant Staphylococcus aureus (MRSA). Silver-containing dressings are available in multiple forms including foam, alginate, and hydrocolloid formulations.
- Cadexomer iodine: This slow-release iodine formulation effectively disrupts biofilm, absorbs exudate, and provides sustained antimicrobial activity.
- Manuka honey dressings: Medical-grade Manuka honey has a unique combination of osmotic, hydrogen peroxide-mediated, and methylglyoxal-mediated antimicrobial properties that are effective against biofilm and drug-resistant organisms.
- PHMB (Polyhexamethylene biguanide): A broad-spectrum antiseptic that disrupts bacterial cell membranes, effective against both planktonic bacteria and biofilm.
Phage Therapy
Bacteriophage therapy — the use of viruses that specifically target and kill bacteria — is an emerging frontier in the treatment of antibiotic-resistant diabetic foot infections. While still largely experimental in the Western world, phage therapy has been used compassionately in cases where all antibiotic options have been exhausted, with some remarkable success stories. Clinical trials are currently underway to establish its safety and efficacy more formally.
Advanced Treatment 6: Cellular and Regenerative Medicine Approaches
The frontier of regenerative medicine is rapidly expanding its reach into diabetic wound care, offering therapies that go beyond simply treating the wound surface to actually rebuilding and regenerating damaged tissue from the inside out.
Stem Cell Therapy
Stem cells — particularly mesenchymal stem cells (MSCs) derived from bone marrow, adipose tissue, or umbilical cord blood — have enormous potential in diabetic wound healing. MSCs promote healing through multiple mechanisms: they differentiate