Introduction: The Growing Challenge of Diabetic Foot Wounds
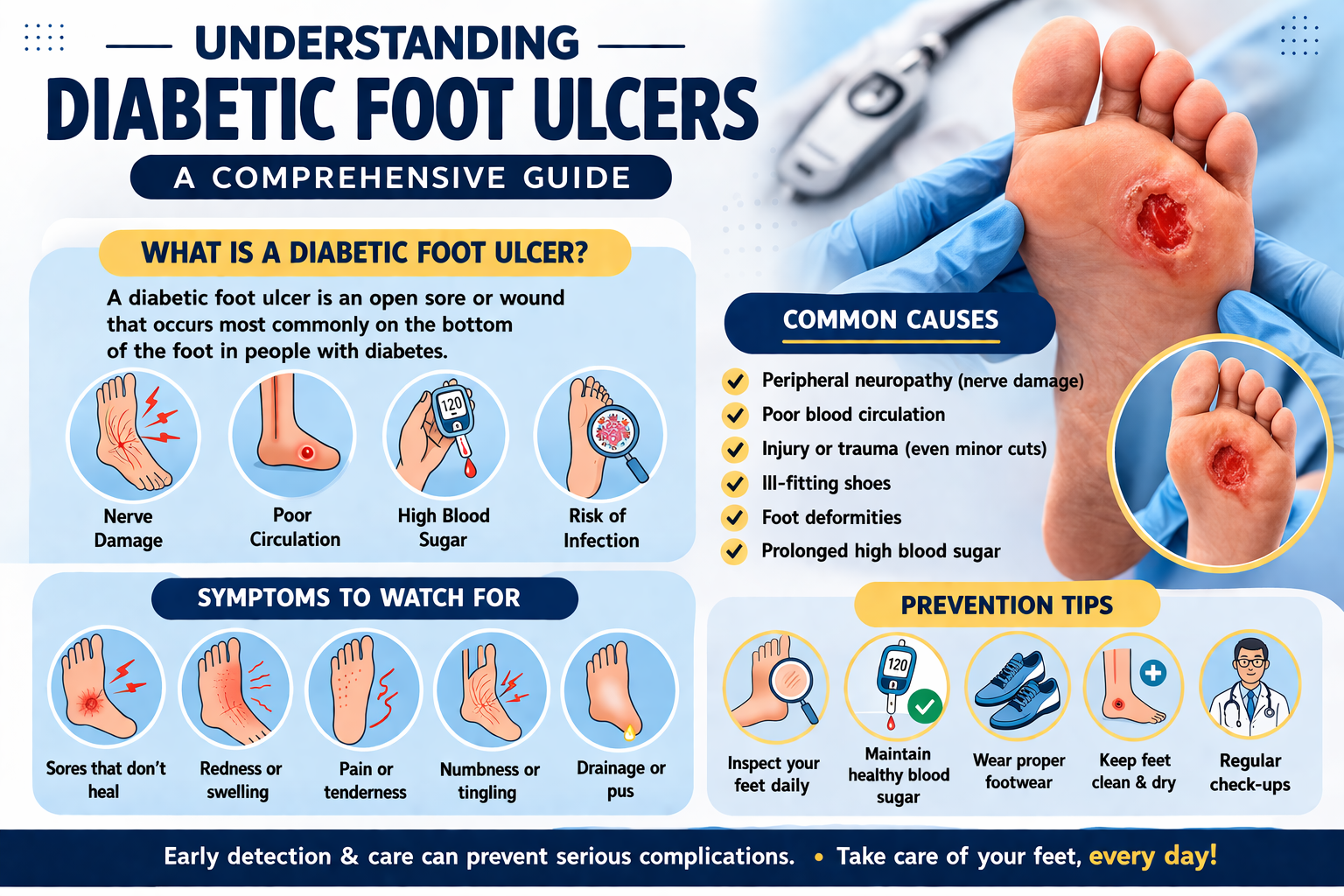
Diabetic foot wounds represent one of the most serious and costly complications of diabetes mellitus, affecting millions of people worldwide. These wounds, which range from superficial ulcerations to deep tissue infections involving bone, are notoriously difficult to heal and carry an alarming risk of amputation. In fact, diabetes is the leading cause of non-traumatic lower limb amputations globally, with a new amputation occurring somewhere in the world every 20 seconds due to diabetes-related complications.
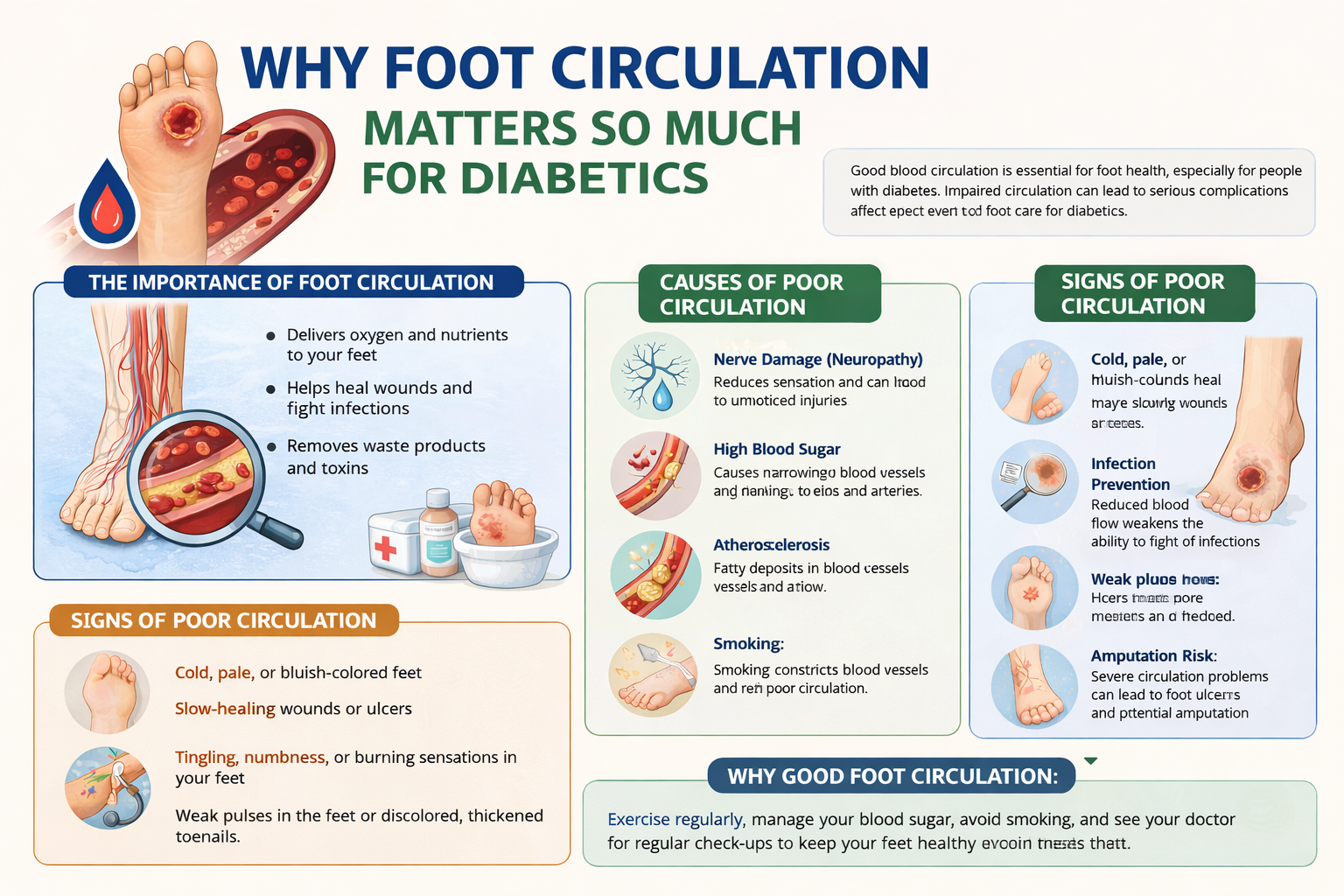
The underlying mechanisms that make diabetic foot wounds so challenging are multifactorial. Peripheral neuropathy causes patients to lose protective sensation, meaning injuries often go unnoticed until they become severely infected. Peripheral arterial disease restricts blood flow, depriving tissues of the oxygen and nutrients needed for healing. Impaired immune function makes diabetic patients more susceptible to infections, and metabolic dysregulation disrupts nearly every aspect of the wound healing cascade.
Fortunately, the landscape of diabetic foot wound care has changed dramatically in recent decades. Advances in molecular biology, bioengineering, regenerative medicine, and wound care technology have produced a remarkable array of treatment options that go far beyond simple dressing changes and debridement. This article explores the most advanced and promising treatments currently available for diabetic foot wounds, offering hope for improved healing outcomes and limb preservation.
Understanding Why Diabetic Foot Wounds Are Different
Before diving into advanced treatments, it is essential to understand why diabetic foot wounds behave differently from ordinary wounds. The healing process in healthy individuals follows a predictable sequence of phases: hemostasis, inflammation, proliferation, and remodeling. In diabetic patients, this process is disrupted at virtually every stage.
The Pathophysiology of Impaired Healing
Chronic hyperglycemia triggers a cascade of harmful biochemical changes. Advanced glycation end products (AGEs) accumulate in tissues, stiffening blood vessel walls and impairing microvascular function. Reactive oxygen species are produced in excess, creating oxidative stress that damages cells and impairs growth factor signaling. Neutrophils and macrophages — the immune cells responsible for clearing bacteria and initiating tissue repair — become dysfunctional, failing to mount adequate responses to infection.
Wound healing also depends heavily on growth factors such as vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), and fibroblast growth factor (FGF). In diabetic wounds, these growth factors are produced in insufficient quantities, and their receptors are often downregulated. The result is a wound that becomes “stuck” in a chronic inflammatory state, unable to progress to proliferation and tissue regeneration.
Classification and Risk Stratification
Proper classification of diabetic foot wounds is critical for guiding treatment decisions. Several validated systems exist, including the Wagner Classification System, the University of Texas Wound Classification System, and the WIfI (Wound, Ischemia, foot Infection) classification. These systems assess wound depth, degree of ischemia, and presence of infection to determine overall limb threat and guide the urgency and type of intervention required.
The Foundation: Comprehensive Wound Bed Preparation
Before any advanced treatment can be effective, proper wound bed preparation is essential. The TIME framework — addressing Tissue, Infection/inflammation, Moisture balance, and Edge — provides a systematic approach to creating the optimal wound environment.
Sharp Surgical Debridement
Debridement — the removal of necrotic, devitalized, and infected tissue — remains the cornerstone of diabetic foot wound management. Sharp surgical debridement, performed by trained clinicians using scalpels, curettes, and scissors, is widely regarded as the most effective method. It rapidly removes necrotic burden, stimulates the wound edge, reduces bacterial biofilm, and converts a chronic wound into an acute one, reinvigorating the healing response.
Regular debridement, performed at frequent intervals, has been shown to significantly improve healing rates in diabetic foot ulcers. Studies have demonstrated that wounds that receive sharp debridement more frequently have higher rates of closure and lower rates of amputation compared to those managed with less aggressive approaches.
Hydrosurgical and Ultrasonic Debridement
For wounds with significant devitalized tissue or heavy biofilm burden, advanced debridement technologies offer additional benefits. Hydrosurgical debridement systems, such as the VERSAJET, use a high-pressure water jet to precisely remove necrotic tissue while preserving viable structures. This technology is particularly useful in anatomically complex areas of the foot where traditional sharp debridement carries greater risk of inadvertent damage to tendons and neurovascular structures.
Low-frequency ultrasonic debridement is another powerful tool, using sound waves to disrupt bacterial biofilm and stimulate cellular activity in the wound bed. Clinical evidence suggests ultrasonic debridement can reduce bacterial burden, enhance growth factor activity, and accelerate healing in chronic diabetic foot ulcers.
Offloading: The Non-Negotiable Component of Healing
Regardless of which advanced treatments are employed, no diabetic foot ulcer will heal if excessive pressure continues to be applied to the wound site. Offloading — redistributing or eliminating pressure from the wound — is considered by most wound care experts to be the single most important intervention in the management of neuropathic diabetic foot ulcers.
Total Contact Casting
Total contact casting (TCC) is widely recognized as the gold standard for offloading plantar diabetic foot ulcers. A TCC is a specially molded fiberglass or plaster cast that distributes weight evenly across the entire plantar surface of the foot, dramatically reducing peak plantar pressure at the wound site. Clinical trials consistently show that TCC achieves healing rates of 80–90% in neuropathic plantar ulcers, outperforming removable cast walkers and other offloading devices.
Despite its proven efficacy, TCC remains underutilized in clinical practice, largely due to concerns about patient compliance, cost, and skill requirements for proper application. Efforts to train more clinicians in TCC application and to develop prefabricated alternatives that approach TCC’s effectiveness are ongoing.
Removable Cast Walkers and Specialized Footwear
Removable cast walkers (RCWs) and instant total contact casts — created by rendering an RCW irremovable — offer practical alternatives for patients who cannot tolerate TCC. Custom-molded orthotic insoles and therapeutic footwear play an important role in the longer-term prevention of recurrence after wound healing, reducing plantar pressure at vulnerable sites.
Revascularization: Restoring Blood Flow for Healing
In diabetic patients with significant peripheral arterial disease (PAD), wound healing cannot occur without adequate restoration of blood flow. Vascular assessment using ankle-brachial index (ABI), toe-brachial index, transcutaneous oxygen pressure (TcPO2), and duplex ultrasound guides decisions about the need for and feasibility of revascularization.
Endovascular Interventions
Percutaneous transluminal angioplasty (PTA), with or without stenting, has become the preferred revascularization strategy in many diabetic patients due to its minimally invasive nature. Modern endovascular techniques, including drug-eluting balloons, atherectomy devices, and dedicated below-the-knee intervention systems, have dramatically expanded the ability to treat complex, multi-level arterial disease that is common in diabetic patients. Successful endovascular revascularization significantly increases rates of wound healing and limb salvage.
Surgical Bypass
For patients with anatomical patterns of disease not amenable to endovascular treatment, open surgical bypass using autologous vein grafts remains an important option. Distal bypass procedures to tibial and pedal vessels — once considered technically challenging — are now routinely performed at specialized limb salvage centers, with outcomes demonstrating high rates of wound healing and limb preservation in carefully selected patients.
Advanced Wound Dressings and Topical Therapies
The development of advanced wound dressings has moved far beyond simple gauze and bandages. Modern dressings are engineered to create and maintain the optimal wound environment, manage exudate, combat infection, and actively promote healing.
Silver-Containing and Antimicrobial Dressings
Infection is a major complication of diabetic foot wounds, and antimicrobial dressings play a key role in managing wound bioburden. Silver-containing dressings release silver ions that have broad-spectrum antimicrobial activity against bacteria including methicillin-resistant Staphylococcus aureus (MRSA) and Pseudomonas species. Iodine-based dressings, honey-impregnated dressings (particularly Manuka honey), and polyhexamethylene biguanide (PHMB) dressings offer additional antimicrobial options with distinct properties suited to different wound types.
Foam, Hydrocolloid, and Hydrofiber Dressings
Moisture balance is critical in wound healing — wounds that are too dry or too wet heal poorly. Foam dressings provide excellent exudate absorption and thermal insulation, making them suitable for moderately to highly exuding wounds. Hydrocolloid dressings maintain a moist wound environment, support autolytic debridement, and protect the wound from external contamination. Hydrofiber dressings such as Aquacel absorb large amounts of exudate and convert it into a gel, managing moisture while reducing maceration of the periwound skin.
Collagen-Based Dressings
Collagen dressings donate exogenous collagen to the wound environment, stimulating fibroblast activity and providing a scaffold for new tissue formation. They also act as sacrificial substrates for matrix metalloproteinases (MMPs), which are chronically elevated in diabetic wounds and destroy growth factors and the extracellular matrix needed for healing. By absorbing excess MMPs, collagen dressings help restore a more conducive biochemical environment for repair.
Negative Pressure Wound Therapy (NPWT)
Negative pressure wound therapy — also known as vacuum-assisted closure (VAC) therapy — has become one of the most widely adopted advanced treatment modalities for complex diabetic foot wounds. The technology involves applying a sealed foam or gauze dressing to the wound, connected to a vacuum pump that creates sub-atmospheric pressure across the wound surface.
Mechanisms of Action
NPWT achieves its therapeutic effects through multiple mechanisms. Negative pressure reduces wound edema by drawing fluid and inflammatory exudate away from the wound bed. It increases local blood flow and promotes angiogenesis. It applies mechanical strain to wound edge cells, stimulating proliferation and migration. It removes bacterial load and inhibits the formation of new biofilm. Together, these effects accelerate granulation tissue formation and wound contraction, preparing the wound for either spontaneous closure or surgical reconstruction.
Clinical Evidence and Applications
Multiple randomized controlled trials have demonstrated that NPWT significantly increases the proportion of diabetic foot ulcers that achieve complete healing, reduces healing time, and lowers the rate of secondary amputations compared to standard wound care. NPWT is particularly valuable after surgical debridement, partial foot amputation, and in post-surgical wounds following revascularization procedures. Newer NPWT systems with instillation and dwell capabilities — which cyclically deliver and remove irrigation solutions — show even greater promise for infected wounds with heavy biofilm burden.
Bioengineered Skin Substitutes and Cellular Therapies
One of the most exciting frontiers in diabetic foot wound treatment is the development of bioengineered skin substitutes and cellular therapies. These products aim to replace the cellular and structural components that are deficient in chronic diabetic wounds, essentially providing the biological signals needed to restart the healing process.
Bilayered Cellular Matrix (Apligraf)
Apligraf is a living bilayered skin substitute containing allogeneic human keratinocytes and fibroblasts embedded in a bovine collagen matrix. It delivers growth factors, cytokines, and extracellular matrix components directly to the wound bed. Clinical trials have shown that Apligraf significantly increases healing rates in diabetic foot ulcers compared to standard care, particularly in wounds that have failed to respond to conventional treatment.
Dermal Regeneration Templates
Products such as Dermagraft, a cryopreserved human fibroblast-derived dermal substitute, and Integra Dermal Regeneration Template, an acellular bilayer matrix derived from bovine collagen and shark chondroitin sulfate, provide scaffolding for tissue regeneration in complex wounds. These matrices are particularly useful in wounds with exposed tendons, bone, or joint capsules, where conventional healing is unlikely without tissue coverage.
Amniotic Membrane Products
Human amniotic membrane-derived products represent a rapidly growing category of wound care biologics. Amniotic membrane contains a rich array of growth factors, cytokines, and anti-inflammatory mediators that can powerfully stimulate healing. Products such as EpiFix and Grafix have demonstrated impressive results in clinical trials, with some studies showing complete healing of chronic diabetic foot ulcers in 50–60% of treated patients compared to 30–35% with standard care.
Growth Factor Therapies
Since growth factor deficiency is a central feature of impaired diabetic wound healing, exogenous delivery of growth factors represents a logical and scientifically compelling therapeutic strategy.
Becaplermin (Regranex)
Becaplermin is a recombinant human platelet-derived growth factor (rhPDGF-BB) available as a topical gel. It is the only FDA-approved growth factor product specifically indicated for diabetic foot ulcers. Clinical trials demonstrated that becaplermin increased complete wound closure rates compared to placebo gel. However, its use has been somewhat limited by concerns about cost, a potential (though controversial) association with increased cancer risk at high doses, and the requirement for a well-vascularized wound bed for efficacy.
Emerging Growth Factor Strategies
Ongoing research is exploring gene therapy approaches to sustained growth factor delivery, including plasmid-based delivery of VEGF and FGF genes directly into ischemic diabetic foot tissues to stimulate therapeutic angiogenesis. Early clinical trials have shown promising results in patients with critical limb ischemia, and this approach may become an important adjunct to conventional revascularization in the future.
Platelet-Rich Plasma (PRP) Therapy
Platelet-rich plasma therapy involves processing a small sample of the patient’s own blood to concentrate platelets and the growth factors they contain — including PDGF, VEGF, transforming growth factor-beta (TGF-β), and epidermal growth factor (EGF) — and applying this concentrate directly to the wound bed.
How PRP Works
When activated PRP is applied to a wound, platelets degranulate and release their growth factor payload, creating a localized supraphysiological concentration of signaling molecules that can stimulate cell migration, proliferation, angiogenesis, and matrix synthesis. Because PRP is autologous, there is no risk of disease transmission or immune rejection, making it an attractive option for many patients.
Clinical Evidence
Multiple systematic reviews and meta-analyses have concluded that PRP therapy significantly improves healing rates in diabetic foot ulcers compared to standard care, with several studies reporting complete healing rates two to three times higher with PRP treatment. While the quality of evidence is variable and larger randomized controlled trials are needed, PRP has gained widespread acceptance as a valuable adjunctive treatment, particularly in wounds that have stalled despite conventional management.
Hyperbaric Oxygen Therapy (HBOT)
Hyperbaric oxygen therapy involves placing patients in a pressurized chamber where they breathe 100% oxygen at pressures greater than atmospheric. This dramatically increases the partial pressure of oxygen dissolved in blood plasma, allowing oxygen to reach ischemic wound tissues that are inaccessible to red blood cell-bound oxygen.
Mechanisms and Benefits
The hyperoxygenation achieved with HBOT