Understanding Diabetic Foot Ulcers: A Comprehensive Guide
Diabetes is one of the most prevalent chronic conditions in the world, affecting hundreds of millions of people globally. While much attention is given to managing blood sugar levels and preventing heart disease, one of the most serious and often overlooked complications of diabetes is the development of foot ulcers. Diabetic foot ulcers are open sores or wounds that occur in approximately 15% of patients with diabetes, and they remain one of the leading causes of hospitalization and lower limb amputation worldwide.
If you or someone you love is living with diabetes, understanding the causes, recognizing the symptoms early, and knowing the available treatment options can make the difference between full recovery and life-altering complications. This comprehensive guide will walk you through everything you need to know about diabetic foot ulcers — from why they develop to how they are treated and prevented.
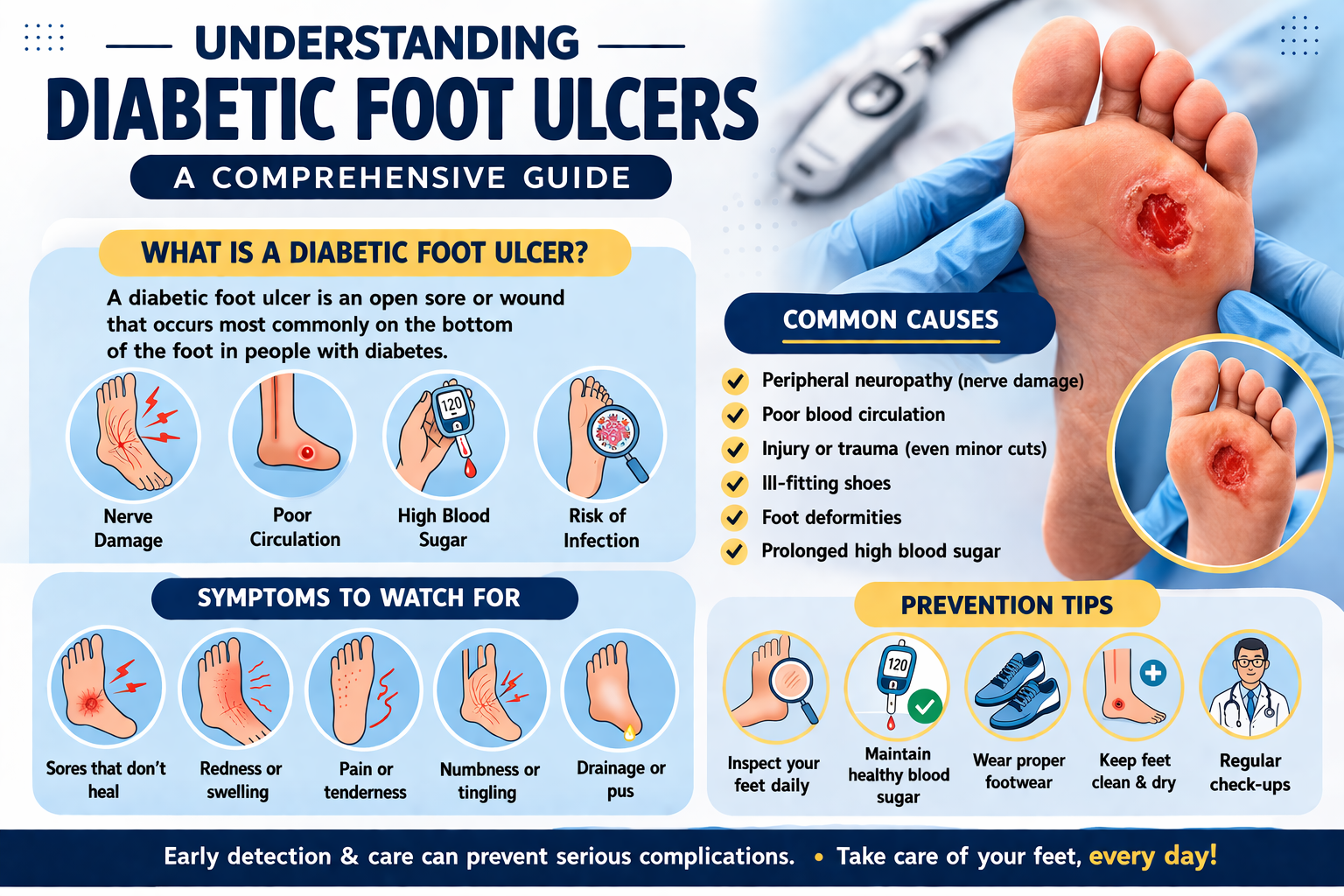
What Is a Diabetic Foot Ulcer?
A diabetic foot ulcer is a break in the skin or a deep wound that occurs on the foot of a person with diabetes. These ulcers most commonly develop on the bottom of the foot, particularly under the big toe and the balls of the feet. However, they can occur anywhere on the foot or lower leg.
Unlike ordinary cuts or wounds that heal within a few days, diabetic foot ulcers are notoriously slow to heal due to the complex physiological changes caused by diabetes. In many cases, these ulcers can persist for weeks or even months, becoming infected and potentially spreading to the bone. When left untreated or poorly managed, diabetic foot ulcers can lead to gangrene and ultimately require amputation of a toe, foot, or even the lower leg.
The good news is that with proper education, early detection, and timely medical care, the majority of diabetic foot ulcers can be successfully treated and, in many cases, prevented altogether.
Causes of Diabetic Foot Ulcers
Diabetic foot ulcers do not appear out of nowhere. They are the result of a combination of factors that make the feet of diabetic patients particularly vulnerable to injury and poor healing. Understanding these underlying causes is essential to effective prevention and treatment.
1. Peripheral Neuropathy (Nerve Damage)
One of the primary causes of diabetic foot ulcers is peripheral neuropathy — a type of nerve damage that is an extremely common complication of both Type 1 and Type 2 diabetes. When blood sugar levels remain elevated over a long period of time, they cause damage to the nerves throughout the body, particularly those in the feet and legs.
Peripheral neuropathy leads to a loss of sensation in the feet. This means that a person with diabetes may not feel pain, heat, or pressure the way a healthy person would. As a result, small injuries such as blisters, cuts, or pressure sores can go completely unnoticed. Without pain as a warning signal, these minor wounds are left unattended and can quickly worsen into full-blown ulcers.
2. Poor Circulation (Peripheral Arterial Disease)
Diabetes significantly increases the risk of peripheral arterial disease (PAD), a condition in which the arteries that supply blood to the legs and feet become narrowed or blocked due to a buildup of fatty deposits. Poor circulation means that the feet receive an inadequate supply of oxygen and nutrients, both of which are essential for healing wounds.
When a small cut or sore develops on the foot of someone with compromised circulation, the body simply does not have the resources to repair the tissue effectively. This leads to prolonged healing times, increased susceptibility to infection, and a higher likelihood of developing a chronic, non-healing ulcer.
3. High Blood Sugar Levels (Hyperglycemia)
Chronically elevated blood sugar levels — the hallmark of poorly controlled diabetes — directly impair the body’s ability to heal. High glucose levels interfere with the function of white blood cells, which are the body’s primary defense against infection. They also damage blood vessels and nerves, compounding the problems of neuropathy and poor circulation.
Additionally, high blood sugar creates an environment in which bacteria thrive, making any wound on the foot of a diabetic patient far more susceptible to infection than it would be in a non-diabetic individual.
4. Foot Deformities and Abnormal Pressure
Many people with diabetes develop structural foot deformities over time, such as hammertoes, bunions, or Charcot foot — a condition that causes the bones of the foot to weaken and fracture, sometimes changing the shape of the foot dramatically. These deformities create areas of abnormal pressure on the foot when walking or standing.
Repeated pressure or friction on the same spot causes calluses to form. While calluses may seem harmless, in diabetic patients they can mask underlying tissue damage and eventually break down to form ulcers. Wearing ill-fitting shoes further exacerbates this problem by creating friction and pressure points that can easily lead to skin breakdown.
5. Trauma and Minor Injuries
Because of neuropathy and reduced sensation, diabetic patients are at risk of injuring their feet without realizing it. Walking barefoot, stepping on sharp objects, wearing new or tight shoes, or even clipping toenails too aggressively can result in small wounds that go unnoticed and untreated until they develop into serious ulcers.
6. Immune System Dysfunction
Diabetes weakens the immune system, making the body less effective at fighting off bacteria and other pathogens. This means that even a superficial wound can quickly become infected, and once an infection takes hold, it is much harder for a diabetic patient to overcome it. Infections that would be relatively minor in healthy individuals can rapidly become life-threatening in people with diabetes.
7. Lifestyle and Risk Factors
Certain lifestyle factors significantly increase the risk of developing diabetic foot ulcers. These include:
- Smoking: Tobacco use constricts blood vessels and further impairs circulation in the feet and legs.
- Obesity: Excess body weight increases pressure on the feet and worsens insulin resistance.
- Sedentary lifestyle: Lack of physical activity contributes to poor circulation and worse blood sugar control.
- Alcohol consumption: Excessive alcohol use can worsen neuropathy and impair wound healing.
- Long duration of diabetes: The longer a person has had diabetes, the greater their cumulative risk of developing complications including foot ulcers.
Symptoms of Diabetic Foot Ulcers
Recognizing the symptoms of a diabetic foot ulcer early is critical to preventing serious complications. Unfortunately, because neuropathy causes a loss of sensation, many people with diabetes do not feel pain from an ulcer and may not notice it until it has become quite advanced. This makes regular foot inspection an essential habit for all diabetic patients.
Early Warning Signs
Before a full ulcer develops, there are often early warning signs that something is wrong with the foot. These include:
- Redness or discoloration: Areas of redness, pink, or dark discoloration on the skin of the foot can indicate early tissue damage or infection.
- Swelling: Localized or generalized swelling in the foot or ankle may signal underlying inflammation or infection.
- Warmth: A specific area of the foot that feels warmer than surrounding tissue may indicate increased blood flow to an area of injury or infection.
- Calluses or hardened skin: Thick calluses, particularly over pressure points, can be a precursor to ulcer formation.
- Skin changes: Dry, cracked skin, changes in skin color, or skin that appears shiny and taut can all be warning signs.
- Tingling or burning: Some patients experience unusual sensations such as tingling, burning, or numbness, which may indicate neuropathy progression.
Symptoms of an Active Ulcer
Once an ulcer has formed, the following symptoms may be present:
- Open sore or wound: A visible break in the skin that may appear as a shallow or deep crater, often with irregular edges.
- Drainage or discharge: The ulcer may produce clear, yellow, or greenish fluid. Foul-smelling discharge is a sign of infection.
- Black tissue (eschar): Blackened or dead tissue surrounding or within the ulcer indicates necrosis, a serious condition that requires immediate medical attention.
- Odor: A persistent unpleasant smell coming from the foot can be a sign of infection or tissue death.
- Pain (in some cases): While many diabetic patients do not feel pain due to neuropathy, some may experience discomfort, throbbing, or pain around the ulcer, particularly if infection is present.
- Fever or chills: Systemic symptoms like fever, chills, or feeling generally unwell may indicate that an infection has spread beyond the ulcer site.
Stages of Diabetic Foot Ulcers
Healthcare professionals use classification systems such as the Wagner Grading System to categorize the severity of diabetic foot ulcers. Understanding these stages helps determine the appropriate course of treatment:
- Grade 0: No open sore, but the foot is at high risk due to calluses, deformities, or previous ulcers.
- Grade 1: A superficial ulcer involving only the skin, with no infection or involvement of deeper tissues.
- Grade 2: The ulcer extends deeper into the foot, involving tendons, capsule, or bone.
- Grade 3: Deep ulcer with abscess, osteomyelitis (bone infection), or tendon involvement.
- Grade 4: Gangrene affecting part of the foot, typically a toe or forefoot.
- Grade 5: Extensive gangrene involving the entire foot, often requiring major amputation.
Diagnosis of Diabetic Foot Ulcers
When a patient presents with a suspected diabetic foot ulcer, a healthcare provider will conduct a thorough evaluation to assess the severity of the ulcer, identify any underlying infection, and determine the best course of treatment.
Physical Examination
The doctor will carefully examine the foot, looking at the size, depth, and appearance of the ulcer. They will check for signs of infection, assess the circulation in the foot, and evaluate the degree of neuropathy by testing sensation with a monofilament or tuning fork.
Diagnostic Tests
Several diagnostic tests may be ordered to better understand the ulcer and guide treatment:
- Blood tests: Complete blood count (CBC) to check for signs of infection; HbA1c to assess long-term blood sugar control; and other markers of inflammation.
- Wound culture: A sample of tissue or fluid from the ulcer may be sent to the laboratory to identify the specific bacteria causing infection and determine antibiotic sensitivity.
- X-rays: To check for bone infections (osteomyelitis) or foreign objects in the foot.
- MRI or CT scan: More detailed imaging may be needed to assess the extent of soft tissue or bone involvement.
- Ankle-brachial index (ABI): A simple, non-invasive test to measure blood flow in the legs and assess for peripheral arterial disease.
- Doppler ultrasound or angiography: To assess blood vessel health and circulation in greater detail if PAD is suspected.
Treatment of Diabetic Foot Ulcers
The treatment of diabetic foot ulcers is complex and typically requires a multidisciplinary approach involving podiatrists, endocrinologists, vascular surgeons, wound care specialists, and sometimes infectious disease specialists. The goals of treatment are to heal the ulcer, prevent or treat infection, address underlying causes, and prevent recurrence.
1. Wound Care and Debridement
The cornerstone of diabetic foot ulcer treatment is proper wound care. This involves cleaning the wound, removing dead or infected tissue (a process called debridement), and applying appropriate dressings to promote healing.
Debridement can be performed in several ways, including sharp debridement (using a scalpel or scissors), enzymatic debridement (using topical agents to dissolve dead tissue), mechanical debridement (using wet-to-dry dressings or irrigation), and biological debridement (using medical-grade maggots to clean the wound). Regular debridement is essential because the presence of dead tissue and biofilm (bacterial colonies) significantly impairs wound healing.
2. Offloading — Relieving Pressure
One of the most critical components of diabetic foot ulcer treatment is offloading — reducing or eliminating pressure on the wound. Since most ulcers develop in areas subject to repeated pressure during walking, continued pressure will prevent healing and cause further tissue damage.
Methods of offloading include:
- Total contact casting (TCC): Considered the gold standard for offloading plantar (bottom of foot) ulcers, TCC is a specially molded cast that distributes pressure evenly across the foot.
- Removable cast walkers: Boots or walkers that can be taken off for hygiene but provide pressure relief when worn.
- Therapeutic footwear: Specially designed diabetic shoes and custom orthotics that accommodate foot deformities and distribute pressure more evenly.
- Crutches or wheelchairs: In some cases, complete non-weight-bearing may be necessary.
3. Infection Management and Antibiotics
If the ulcer is infected, prompt antibiotic therapy is essential. The choice of antibiotic will depend on the results of the wound culture and whether the infection is mild, moderate, or severe. Mild infections affecting only the skin may be treated with oral antibiotics on an outpatient basis, while more severe infections involving deeper tissues or bone typically require intravenous antibiotics and hospitalization.
In cases where osteomyelitis (bone infection) is present, prolonged antibiotic therapy — sometimes lasting six weeks or more — may be necessary. In some situations, surgical removal of the infected bone may be required.
4. Blood Sugar Control
Optimizing blood glucose management is a fundamental component of diabetic foot ulcer treatment. As mentioned earlier, high blood sugar levels impair healing and create conditions favorable for bacterial growth. Working closely with an endocrinologist or diabetes specialist to achieve target blood sugar levels is essential for successful wound healing.
This may involve adjusting insulin doses, changing oral diabetes medications, modifying diet, or increasing physical activity (within the limits imposed by the need for offloading).
5. Improving Circulation
If peripheral arterial disease is contributing to poor wound healing, treatment to restore blood flow to the foot may be necessary. This is known as revascularization and can be achieved through:
- Angioplasty: A minimally invasive procedure in which a small balloon is used to open narrowed or blocked arteries.
- Stenting: A small metal tube (stent) is placed in the artery to keep it open after angioplasty.
- Bypass surgery: A surgical procedure that creates a new route for blood flow around a blocked artery using a graft.
Improving blood flow to the foot significantly enhances the body’s ability to heal the ulcer and fight infection.